What is a posterior vitreous detachment?
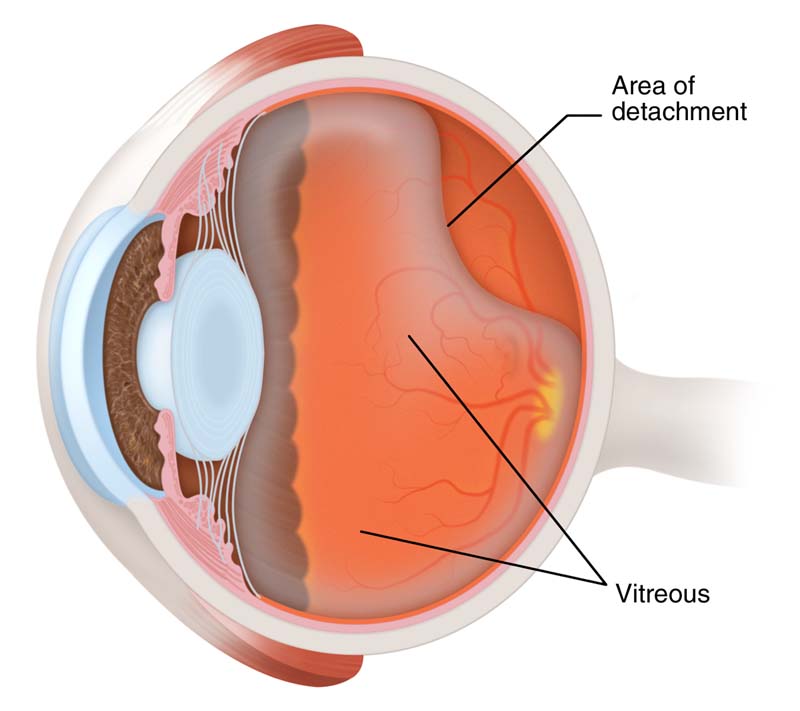
Posterior vitreous detachment (PVD) is a condition of the eye whereby the vitreous gel at the back of the eye separates from the retina.
Studies reveal that it is rare in people under the age of forty years but the risk of PVD increases with the age. However, people over the age 90 have an 86% chance of developing PVD. Cataract surgery also increases the chances of PVD in patients and it may occur within few weeks or months. Its chances are also high in the patients suffering from shortsightedness (myopia). This is because the eyeball is slightly longer in these patients and the vitreous can shrink earlier in life.
- Photopsia (Flashes of light)
- Floaters start to increase suddenly
- A ring of floaters just to the temporal side of the central vision
- Floater complications of PVD
- Blood vessel complications of PVD
- Retinal tear complications of PVD
- Floater complications of PVD
When the vitreous pulls away from the retina, a new floater often appears in the vision. Sometimes it is small and you won’t see it but occasionally it is large and quite noticeable. They are especially noticeable if you cover your other eye, stare at light backgrounds and move your eye side to side.
If the floater stays right in the middle of your vision, it is likely that you will get used to it with time and your brain will “learn” to ignore it. I rarely advocate the use of a laser (laser vitreolysis) to disrupt this type of floater. As the laser can cause more complications than the condition it is trying to treat. In general, I reassure my patients to ignore the floater and monitor for any new floaters that may develop as a result of a retinal tear or retinal detachment (see below).
Blood vessel complication of PVD
Very occasionally the vitreous gel can shrink and pull strongly on a blood vessel on the retina and cause further problems. If the gel pulls on a blood vessel, a small bleed into the vitreous cavity can occur known as a vitreous haemorrhage. This may look like a spider web in the vision. Or, if it disperses, the blood can look like hundreds of small individual floaters. Usually, the blood disappears by itself but you should always get it checked by an ophthalmologist or optometrist to rule out a retinal tear or detachment (see below).
Retinal tear complications of PVD
If the vitreous gel shrinks and pulls strongly on the retina, a small tear can develop. Retinal tears can lead to a retinal detachment when the retina itself pulls away from the back of the eye. This cannot be ignored and needs urgent treatment in most cases.
Treatments to prevent retinal detachment include sealing the retinal tear with a laser (retinopexy) or freezing therapy (cryotherapy).
Treatment of posterior vitreous detachment
Posterior vitreous detachment generally does not require any specific treatment. However, it is appropriate to ensure that there is no retinal tear or detachment. If you are unlucky enough to have a retinal tear or detachment as a result of posterior vitreous detachment, even a prompt diagnosis and treatment cannot prevent loss of vision in that eye.
In case you have any new onset floaters or flashes of light, I recommend seeing your optometrist or ophthalmologist as soon as possible (within 24 to 48 hours). In most cases the ageing phenomenon of posterior vitreous detachment is the cause.
If you have any further questions please feel free to call me on 020 7935 7990 and I would be happy to discuss your needs in person.
![Contact lens infection – Seven ways to avoid one [Infographic]](https://jaheedkhan.co.uk/wp-content/uploads/2016/12/JK-contact-lens-infections-500x383.jpg)

![Five signs that your child may need glasses [Infographic]](https://jaheedkhan.co.uk/wp-content/uploads/2016/11/shutterstock_268867028-500x383.jpg)
{kind=link}
{kind=link}
{kind=link}